Why do we need behaviour change in perioperative care and how to get there?

View of CPOC Behaviour in the Perioperative Team resources hub
This is a personal piece. I have been a surgeon for 30 years. Some behaviours that were normal then would not be tolerated now. To achieve any change, we need to know why change is important and how to change.
CPOC has highlighted that good perioperative care with a connected team and a patient-centred approach leads to large reductions in complications, length of stay, patient regret and unwarranted surgery. Suddenly, an irritating individual who has been tolerated because they have good technical skills no longer seems too important to challenge.
Change means stopping bad behaviours that lead to a poor culture. It also means reinforcing good behaviours that lead to an excellent culture and good team-working.
Evidence of the extent and impact of poor behaviours:
Poor behaviours are common. They have a bad effect on staff health and retention and on patient outcomes. Sexism, racism and bullying are common across the NHS [1,2,3]. A negative culture has been shown to reduce team functioning and disproportionally affects people who feel that they do not belong (including women, LGBTQ+ people, people from the global majority backgrounds and others).
- Co-workers reduce productivity 20% on witnessing rudeness.[4]
- 48% of staff who are recipients of poor behaviour reduce their time at work.[4]
- 30% of women surgeons experience sexual harassment.[1]
- 91% of women doctors experience sexism regularly.[2]
- 17% of staff from BAME background experience discrimination from other staff.[3]
- Poor behaviours mean staff leave or do not perform at their best.
- Many Serious Untoward Incidents for patients have poor team-working as a contributory factor.
- 54% of departments undergoing investigation for poor surgical results demonstrate individual bad behaviours.[5]
What is not readily acknowledged
People may think this is difficult, but in reality:
- It is possible to change behaviours.[6,7]
- Diverse teams work better. This may be because information has to be clear.
- Harassment is illegal.
- The problem with bad behaviour is the impact on the recipient, not whether this was intended, so there is no need to try to find proof of intent, except for the egregious cases.[6]
- No one is too important to be polite.
- Good behaviours create a good culture.
Should we all just report more?
We need reporting structures in place for egregious behaviours. Unfortunately, disciplinary procedures can be traumatic and lengthy - the Royal College of Obstetricians and Gynaecologists describes reporting as potentially a ‘nuclear option’.[6] Prevention through raising awareness and education of the workforce is better. Programmes suggesting “Zero tolerance” for poor behaviour are not recommended because they can create a focus on the binary decision of whether something is reportable rather than improving behaviours in general.[8]
For other levels of poor behaviour (see Figure 1) interventions based on “awareness” or a “cup of coffee conversation” are effective.
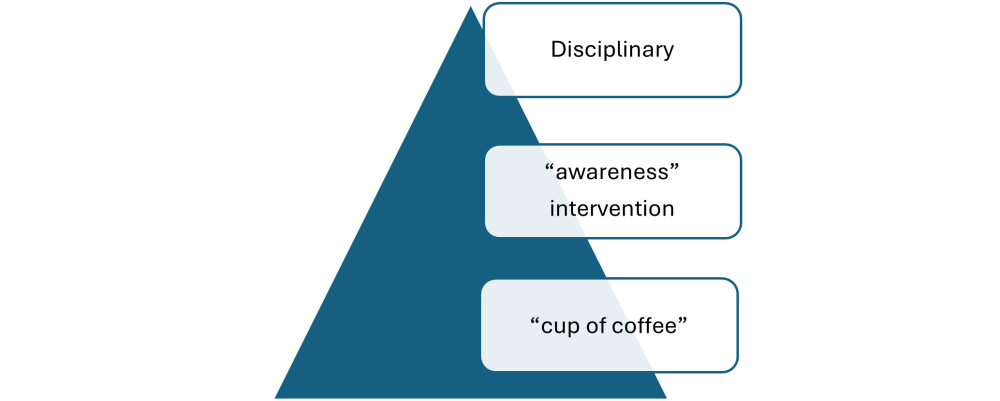
Figure 1: Levels of poor behaviour and possible interventions
Why do some people behave badly and what works to get change?
In 2016, as a Council member, I was lead author for the Royal College of Surgeons of England’s guidance ‘Avoiding unconscious bias: a guide for surgeons’[6]. This lists what counts as bullying and explains how to behave. Many people have never been taught how to interact. We may mistake things being done differently for things being done worse. The human brain is alert to differences. This is why we need to be clear and explain what we expect at work. Many perpetrators of poor behaviours do not realise how they are perceived. They may act badly when they feel patient care is being compromised. They may also have trigger moments that are relatively short, but other staff then end up tiptoeing around, trying to appease them at other times. Some need compassion. Burnout is common and makes people feel blunted to the effect of their actions. Many people have challenges in their home life. We should expect each person to be “good enough” each day, not perfect. The culture of the working environment should include respect and professional ways of working. The Royal Australasian College of Surgeons led a successful “Respect” campaign[9]. The Royal College of Surgeons of Edinburgh has resources[10]. This is better for staff retention, staff wellbeing and patient safety.
Suggested individual behaviour change from potential perpetrators:
As Simon Fleming, who led the #HammerItOut initiative to reduce bullying in surgery said, “It starts with me”.
- Many stressful points can be predicted in advance. These could be discussed in the team.
- Feedback should always be about the task not the individual.
- Explain what is required beforehand rather than berating people for not delivering it. The NatSSIPs Team Brief may help.[11]
- Realise that more diverse teams work better – and this requires time to clarify expectations and discuss how to maximise everyone’s contribution. Have a minimum standard of behaviour and a minimum expectation of each other member of staff.
- Be polite to new staff and students.
- Realise that your interpretation of someone else’s behaviour may be wrong – show respect. Be clear about what needs to happen to get the best result for the patient. We can all learn.
- As a supervisor, ask what they need, give opportunities based on their role and stretch targets based on the potential of their role.
Suggested individual behaviour change from other staff:
Initiatives that improve behaviour should be promoted, for example:
- Be clear about each person’s name and role
- Empower the workforce to call out bad behaviour
- Foster Allyship
- Promote Active Bystander training
- Use the Association of Anaesthetists’ resources eg “I notice you are stressed, is there anything the team can do to help?”[12]
- Plan for “Cup of coffee conversations” (a senior colleague taking someone for a cup of coffee to discuss how their behaviour may have been perceived). This involves asking someone if they are OK – if they have behaved badly, listening and stating the minimum level of behaviour. The Royal Australasian College of Surgeons has an App for this.[13]
Suggested organisational actions:
- Meet, work and train across professional groups and boundaries (team training)
- Encourage meetings that welcome discussion
- Work with staff to improve team-working
- Instil education, especially around team-working and expected behaviours (eg embedding NatSSIPs and allowing staff to focus during the swab and instrument count).[14]
- Have clear reporting mechanisms
- Change leadership practices to welcome each member of the team.
- Have clarity about processes, standards and expectations
- Identify patterns of behaviours and stress
- Reduce stress
- Set up standard care pathways with staff - and explain the key points where senior clinicians should be involved
- Have inclusive visible leadership
- Follow up on reports suggesting where change is needed
Other industries:
I am hopeful that behaviours can change across perioperative care. Other industries have shown what is possible, by giving clear instructions.
- The railway industry has posters on what constitutes sexual harassment.[15]
- “Considerate Constructors” is a scheme for the construction industry including safety (hard hats, ladders, etc) and respect (no wolf-whistling).[16]
- RCN’s “gloves off” campaign gives staff permission to work in a different way and can be highly effective.[17]
Summary
Behaviours can change – especially across perioperative care. Clarity and respect are key. Action is needed from individuals and from organisations. Improving behaviours leads to a better culture, better team-working and better patient care. We should stop expecting perfection – because this means we are less open to new ideas or to developing all staff. Improving behaviours is work for all of us, not only the ‘bad apples’.[18]
References:
- www.wpsms.org.uk
- https://www.bma.org.uk/advice-and-support/equality-and-diversity-guidance/gender-equality-in-medicine/sexism-in-medicine-report
- https://www.england.nhs.uk/publication/nhs-workforce-race-equality-standard-2022/
- www.civilitysaveslives.com
- https://www.rcseng.ac.uk/standards-and-research/support-for-surgeons-and-services/irm/improving-professionalism/
- RCS England. Avoiding Unconscious bias: a guide for surgeons. 2016. https://www.rcseng.ac.uk/-/media/Files/RCS/Careers-in-surgery/Study-Page/Avoiding-unconscious-bias.pdf at www.rcseng.ac.uk/study
- https://www.rcseng.ac.uk/standards-and-research/standards-and-guidance/good-practice-guides/managing-disruptive-behaviours/
- https://www.bmj.com/content/383/bmj.p2628
- https://www.surgeons.org/respect AND https://www.surgeons.org/about-racs/about-respect/information-and-updates
- https://www.rcsed.ac.uk/professional-support-development-resources/anti-bullying-and-undermining-campaign
- https://cpoc.org.uk/sites/cpoc/files/documents/2022-12/CPOC_NatSSIPs2_TeamBrief_2023.pdf
- https://anaesthetists.org/Home/Wellbeing-support/-KnockItOut-tackling-workplace-bullying-harassment-and-undermining
- Cup of coffee app. For android: https://play.google.com/store/apps/details?id=com.racs.speakup Or apple: https://apps.apple.com/us/app/racs-speak-up/id1437874350?platform=iphone
- https://cpoc.org.uk/guideline/guidelines-resources-guidelines/national-safety-standards-invasive-procedures-natssips
- https://media.raildeliverygroup.com/news/rail-industry-campaign-to-crack-down-on-sexual-harassment
- https://www.considerateconstructors.com/
- https://www.rcn.org.uk/magazines/Action/2022/Jan/How-to-reduce-glove-use-170122
- McNally BMJ https://www.bmj.com/content/383/bmj.p2628
